
Medication Titration Schedule Calculator
Select Medication
Current Dose
Titration Schedule
Important: Always follow your doctor's specific guidance. This tool is for informational purposes only.
Why Starting Low and Going Slow Works Better for Your Body
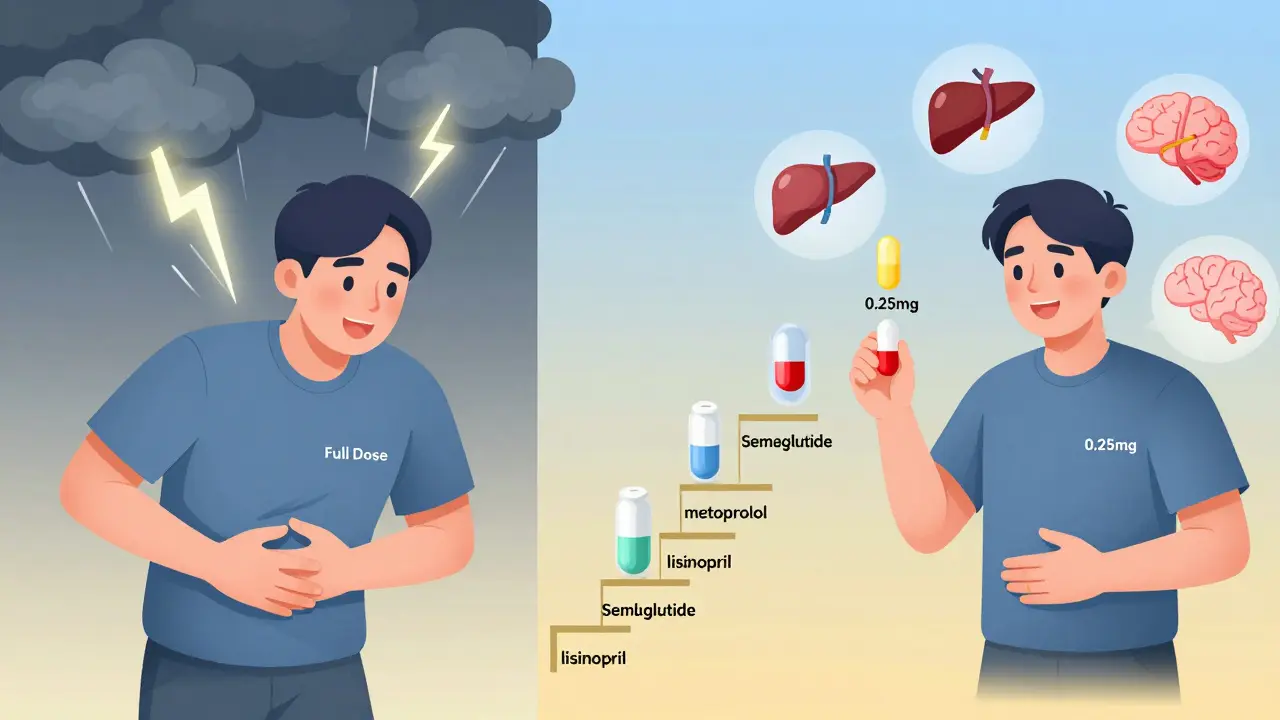
Imagine starting a new medication and feeling sick within days-nausea, dizziness, fatigue-so bad you quit. That’s what happens when you jump straight to the full dose. But if you start at a tiny amount and creep up over weeks or months, your body adapts. That’s slow up-titration, and it’s not just a medical buzzword-it’s the difference between sticking with your treatment and giving up.
Take GLP-1 agonists like semaglutide. At full dose, nearly half of users get severe nausea. But when started at 0.25mg once a week and slowly increased over 16 to 20 weeks, that number drops to less than 20%. The same pattern holds for beta-blockers in heart failure, ACE inhibitors for high blood pressure, and even some antidepressants. It’s not that the drug is weaker at first-it’s that your body gets used to it.
How Slow Up-Titration Actually Changes Your Body
It’s not magic. It’s biology. When you take a new drug, especially one that affects your nervous system or hormones, your body doesn’t just accept it. It reacts. Your receptors get overwhelmed. Your gut panics. Your blood pressure drops too fast. Slow up-titration gives your body time to adjust.
For example, beta-blockers like metoprolol block adrenaline receptors. If you start at 100mg, your heart rate crashes, you feel faint, and you might quit. But if you start at 6.25mg twice daily and double every two weeks, your receptors gradually downregulate. Your body learns to function with less adrenaline. The result? You get the same heart protection without the crash.
This isn’t just theory. A 1984 study in the Journal of the American College of Cardiology found that only 12% of heart failure patients could handle the full dose of metoprolol right away. But when titrated slowly, 83% stayed on it. That’s not a small difference-it’s life-changing.
What Slow Up-Titration Looks Like for Common Medications
Not all medications titrate the same way. The schedule depends on how the drug works and how harsh its side effects are.
- GLP-1 agonists (semaglutide, liraglutide): These are the slowest. Semaglutide injections start at 0.25mg weekly for four weeks, then go to 0.5mg for four weeks, then 1mg for four weeks, and finally up to 2.4mg if needed for weight loss. Oral semaglutide follows a 60-day ramp-up: 3mg for 30 days, then 7mg, then 14mg. This isn’t arbitrary-it’s based on how often nausea and vomiting occur at each level.
- Beta-blockers (metoprolol, carvedilol): For heart failure, start at 6.25mg once or twice daily, double every 2-4 weeks. Blood pressure and heart rate are checked at each visit. Most patients reach target dose in 8-12 weeks.
- ACE inhibitors (lisinopril, enalapril): Start at 2.5-5mg daily, double every 2-4 weeks. Watch for cough, dizziness, or rising creatinine. Many patients reach 10-20mg within 6-8 weeks.
- SGLT2 inhibitors (empagliflozin, dapagliflozin): These are different. Studies show they’re safe to start at full dose. No titration needed. That’s why some patients prefer them-they skip the slow climb.
The key? It’s not one-size-fits-all. Your doctor picks the schedule based on your health, age, kidney function, and what side effects you’ve had before.
Why People Quit-and How to Stay on Track
Even with slow titration, people drop out. Why? Because it’s frustrating. You start feeling better after a few weeks, but you’re still on a low dose. You think, “Why am I not getting results yet?” Then you miss a dose. Or you skip a follow-up. And suddenly, you’re off the medication.
A 2021 meta-analysis in JAMA Internal Medicine found that slow titration improves adherence by 37% compared to starting at full dose. But 23% of patients still miss at least one dose change per month. That’s a lot.
Here’s how to beat that:
- Use a pill organizer labeled with dates and doses.
- Set phone reminders for dose changes and doctor visits.
- Track symptoms in a notebook or app. Note when nausea starts, when dizziness fades. That helps your doctor decide if it’s time to increase.
- Know the 2-week rule: If side effects last longer than two weeks at your current dose, call your provider. Don’t wait. Don’t assume it’ll get better on its own.
One patient on Reddit shared: “Starting semaglutide at 0.25mg saved me. When I tried skipping ahead, I threw up for three days straight and quit. The slow start? I barely noticed anything.” That’s the story behind the science.
When Slow Titration Doesn’t Work-And When It’s Not Needed
Slow titration isn’t for every drug. Some medications are safe to start at full dose.
SGLT2 inhibitors like Jardiance and Farxiga? Studies show no extra benefit from titration. In fact, a 2023 trial called DIAMOND found full-dose initiation was just as safe-and patients reached control faster.
Metformin? For most people, you can start at 500mg daily and ramp up over a few weeks. But if your HbA1c is above 9%, doctors may push faster. Delaying control too long can damage your organs.
And in emergencies? Forget titration. If you’re having a heart attack or severe hypertension, you need fast-acting drugs like labetalol or nitroglycerin. There’s no time to wait.
The rule of thumb? If the side effects are mild and predictable, faster is fine. If they’re strong, sudden, or scary-slow is safer.
What Your Doctor Should Be Doing During Titration
Slow titration isn’t just about you taking pills. It’s a team effort.
Your provider should:
- Give you a written schedule-no vague “increase as tolerated.”
- Check your blood pressure, heart rate, kidney function, and weight at every visit.
- Ask you directly: “What side effects are you having?” not “Are you feeling okay?”
- Use tools like the American Heart Association’s Heart Failure Medication Titration Toolkit, which scores 4.7 out of 5 for clarity.
- Offer telehealth check-ins every 1-2 weeks during the first few months.
A 2022 Mayo Clinic study found doctors spend an average of 12.7 minutes per visit explaining titration. That’s not a waste of time-it’s what makes it work.
If your provider doesn’t give you a clear plan, ask for one. You deserve to know exactly when to increase, what to watch for, and when to call.
The Real Cost: Time, Visits, and Patience
Slow titration takes time. For GLP-1 agonists, it can take 5-6 months to reach the highest dose. For heart failure meds, 3-4 months. That’s a long time to feel like you’re not getting results.
And it costs more. A 2022 analysis in Health Affairs found patients on titration schedules have 2.3 extra doctor visits during the ramp-up phase. That’s time off work, travel, co-pays.
But here’s the trade-off: You’re less likely to end up in the ER because of a bad reaction. You’re less likely to quit. You’re more likely to live longer.
In heart failure, following a strict titration protocol cuts all-cause mortality by 35%, according to Dr. John McMurray’s 2021 study in the European Heart Journal. That’s not just a statistic-it’s someone’s dad, mom, or grandparent still alive because they didn’t rush.
What’s Next? AI, Apps, and Personalized Titration
The future of titration isn’t just paper schedules. It’s smart tech.
Companies like Verily and Novo Nordisk are building AI models that predict how you’ll react to a drug based on your genetics, weight, and past health. Early results show they can predict side effects 28% better than standard methods.
Apps like Omada Health and Medisafe now offer titration reminders, symptom trackers, and even chatbots that answer your questions between visits. One pilot showed a 41% drop in side effect-related dropouts.
But tech doesn’t replace human care. It supports it. The goal isn’t to make titration faster-it’s to make it smoother, more personal, and less lonely.
Final Thought: It’s Not About Speed. It’s About Sustainability.
Medication isn’t a sprint. It’s a marathon. Slow up-titration isn’t about being cautious-it’s about being smart. It’s about giving your body a chance to catch up so you don’t have to quit.
Yes, it takes longer. Yes, you’ll have more appointments. Yes, you’ll feel impatient. But if you stick with it, you’re not just managing side effects-you’re building a treatment that lasts. And that’s the whole point.



kenneth pillet
January 18, 2026 AT 17:27Jodi Harding
January 19, 2026 AT 12:13Stacey Marsengill
January 19, 2026 AT 12:47Selina Warren
January 20, 2026 AT 14:31Naomi Keyes
January 21, 2026 AT 07:40rachel bellet
January 22, 2026 AT 01:56Pat Dean
January 23, 2026 AT 03:07Jay Clarke
January 24, 2026 AT 01:37Robert Davis
January 25, 2026 AT 02:27Jake Moore
January 26, 2026 AT 23:42Max Sinclair
January 28, 2026 AT 11:27Wendy Claughton
January 29, 2026 AT 16:40Ryan Otto
January 30, 2026 AT 13:25