
Here’s the uncomfortable truth: the same oxygen we rush in to save tissue can quietly worsen damage the moment blood flow returns. That’s the paradox at the heart of reperfusion injury. This guide breaks down why it happens, the dose-and-timing traps, and how to use oxygen with intent-so you restore flow without feeding the fire.
What to expect: a simple model for the biology, crisp targets you can use at the bedside, the strongest trial signals, and a practical playbook for emergencies, the ICU, the cath lab, and the OR.
First things first-if you only remember one line, remember this: the role of oxygen in reperfusion injury is about hitting “enough,” not “more.”
- TL;DR: Reperfusion injury is driven by a burst of reactive oxygen species (ROS) when oxygen floods starved tissue. Hyperoxia increases that burst. Target normal oxygenation (SpO2 ~92-96% adults; adjust for COPD and neonates), avoid prolonged FiO2 1.0, and wean fast once perfusion returns.
- Mechanisms: Mitochondrial electron leak, xanthine oxidase, NADPH oxidase, and NO uncoupling spike ROS; this opens the mitochondrial pore, triggers calcium overload, endothelial swelling, and no-reflow.
- Evidence: Normoxic oxygen targets are safe and often better: DETO2X-AMI, AVOID (ACS), SO2S (stroke), ICU-ROX (ICU), and guideline lines from AHA/ASA/ERC/ILCOR/ANZCOR all lean conservative.
- Practice: Titrate to pulse ox, confirm with blood gases, step down FiO2 promptly after ROSC/reperfusion, and consider staged or “controlled” reperfusion in the OR.
- Edge cases: COPD (88-92%), neonates (room air or 21-30% and titrate), hyperbaric oxygen for specific poisoning/embolic syndromes-not routine I/R.
Why Oxygen Flips from Lifesaver to Saboteur
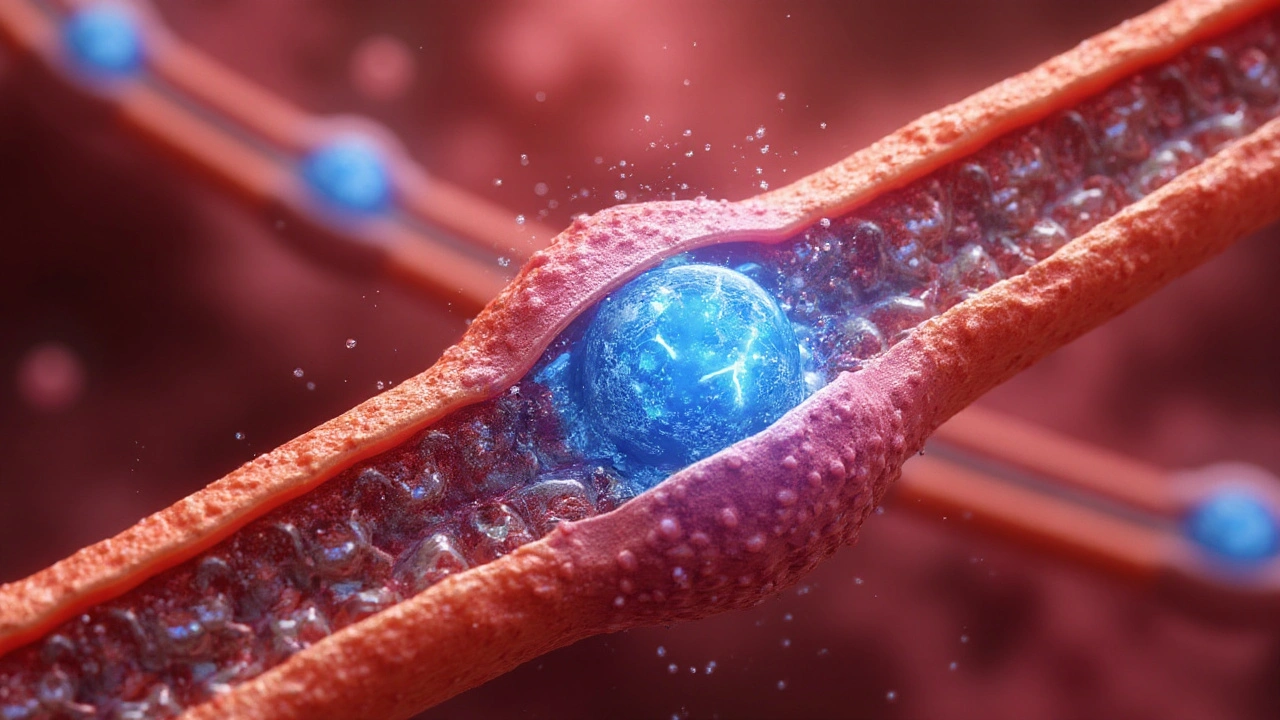
During ischemia, cells build up reduced substrates and pro-oxidant enzymes-think of a spring being wound tight. When blood returns, oxygen turns that spring loose. The first seconds to minutes are the danger zone: high oxygen tension plus primed mitochondria equals a ROS burst that can injure lipids, proteins, and DNA. It also stiffens microvessels, clogs capillaries with leukocytes, and paradoxically keeps parts of tissue dark-the “no-reflow” phenomenon.
Mechanistically, here’s the short list that actually matters at the bedside:
- Mitochondria: Ischemia disrupts the electron transport chain. Reperfusion adds oxygen before the chain is fully “back online,” so electrons leak and form superoxide (O2−). That triggers the mitochondrial permeability transition pore (mPTP) to open, collapsing ATP production and pushing cells toward death.
- Xanthine oxidase: Ischemia converts xanthine dehydrogenase to xanthine oxidase. Reperfusion delivers oxygen, and the enzyme sprays superoxide and hydrogen peroxide.
- NADPH oxidases (NOX): Activated immune cells and endothelium fire up NOX enzymes, adding to the ROS pile and inflaming the microvasculature.
- NO uncoupling: Endothelial nitric oxide synthase can go “uncoupled,” making superoxide instead of nitric oxide. That kills vasodilation when you need it most.
- Calcium overload: Oxygenation restores membrane potentials, calcium rushes in, and mitochondria get hammered-another push toward mPTP opening.
What increases the injury? Two dimensions: oxygen dose (hyperoxia-high FiO2 or PaO2) and time (how long tissue sits in the ROS bath). The quick wins are obvious: avoid sustained FiO2 1.0, target normal saturations, and keep the first 10-30 minutes tidy-because that’s when oxygen does the most good and the most harm.
“Supplemental oxygen is not recommended for adults with suspected acute coronary syndrome who are not hypoxemic (SpO2 ≥ 90%).” - American Heart Association Guidelines, 2020
Why does this show up clinically? Look at MI and stroke trials: when patients weren’t hypoxic, high-dose oxygen didn’t help and sometimes worsened markers of injury. In the ICU, long stretches of hyperoxia correlate with more lung injury and mortality. For neonates, we learned the hard way that excess oxygen drives retinopathy of prematurity; now the standard is room air or low-start titration.
How to Use Oxygen During Reperfusion: A Step‑by‑Step Playbook
Use this when reperfusion is about to happen or has just occurred: ROSC after cardiac arrest, balloon inflation in the cath lab, thrombolysis or thrombectomy for stroke, tourniquet release, or unclamping during surgery.
1) Set a target-not a default.
- Adults: SpO2 92-96% (PaO2 roughly 60-80 mmHg). If you’re using FiO2 1.0 to get there, step it down as soon as the number is stable.
- COPD exacerbation or chronic CO2 retainers: 88-92% to avoid CO2 narcosis.
- Post‑ROSC: 92-96% once you have a waveform and a reliable pulse ox.
- Neonates: Start at room air (term) or 21-30% (preterm) and titrate to minute‑by‑minute targets.
2) Measure, don’t guess.
- Use pulse oximetry continuously; confirm early with arterial blood gas (ABG) after ROSC, after balloon inflation, after limb reperfusion, or post‑clamp release.
- Recheck ABG at 10-20 minutes if you changed FiO2 or ventilation.
- Watch the gradient: if SpO2 is 100% but PaO2 is 250-400 mmHg, you’re in hyperoxia-reduce FiO2.
3) Wean fast, then fine‑tune.
- If you started high (FiO2 1.0 for a hands‑on moment), step down to 0.6 quickly, then to 0.4-0.3 while keeping the saturation in range.
- Use PEEP to maintain oxygenation rather than cranking FiO2.
- In transport, write the saturation target on the handover and say it out loud. Hard stops prevent drift back to FiO2 1.0 “just to be safe.”
4) Match oxygen to flow.
- When flow is restored (ROSC, stent, clamp off), reduce FiO2 unless the saturation drops.
- In low‑flow states (cardiogenic shock), keep targets the same; use flow (pressors, IABP/Impella/ECMO) to meet demand rather than more oxygen.
5) Avoid the early spikes.
- The first 10-30 minutes after reperfusion are peak ROS time. Keep PaO2 in the normal range, correct calcium and pH, and avoid fevers.
- If you have a choice intra‑op, consider controlled or staged reperfusion: release in increments, watch pressures, and prevent a pressure/oxygen surge.
6) Bundle protective moves.
- Temperature: strict normothermia after ROSC or major reperfusion events.
- Glucose: avoid big swings-hyperglycemia amplifies oxidative stress.
- Hemoglobin: correct severe anemia but avoid off‑target transfusions; both anemia and hyperoxia worsen ROS dynamics.
7) Document your target and the plan to wean.
- Write: “SpO2 target 92-96%; reduce FiO2 stepwise as tolerated; ABG in 20 min.” Clear notes stop well‑meaning escalations later.
Real-World Cases, Evidence Signals, and a Quick Reference Table
Case 1: STEMI in the cath lab. He’s normoxic (SpO2 97% on room air). You stent the LAD. Instead of oxygen “just in case,” you leave him on room air, monitor, and only give oxygen if SpO2 dips. Why? DETO2X‑AMI (NEJM 2017) showed no benefit to routine oxygen in normoxemic MI. The AVOID trial (Circulation 2015) even hinted at harm (larger infarct size) with high‑flow oxygen in non‑hypoxic STEMI.
Case 2: Out‑of‑hospital cardiac arrest (ROSC). Paramedics arrive with FiO2 1.0 and SpO2 100%. ABG shows PaO2 280 mmHg. You drop FiO2 to 0.4, keep SpO2 94-96%, and maintain normothermia. This aligns with AHA/ILCOR/ERC guidance: avoid hyperoxia after ROSC and target normal oxygenation.
Case 3: Ischemic stroke (no hypoxia). She’s 96% on room air while you push for thrombectomy. You don’t add oxygen. The SO2S trial (JAMA 2017) found routine oxygen didn’t improve outcomes in non‑hypoxic stroke. AHA/ASA guidelines say the same: treat hypoxia, not normal sats.
Case 4: COPD exacerbation. He’s at 86%. You give low‑flow oxygen and aim for 88-92%, not 100%. That avoids CO2 retention while still fixing hypoxemia and limiting ROS load during any emergent reperfusion.
Case 5: Tourniquet release in ortho. You plan a staged release, low‑normal FiO2, and ABG 10 minutes later. This reduces the oxygen/calcium surge that can tank hemodynamics and worsen muscle injury.
Where’s the line on adjuncts?
- Ischemic conditioning (pre/post/remote) can blunt reperfusion injury in some settings, especially in cardiac surgery. Translation to routine MI care has been mixed.
- Antioxidants (vitamin C, N‑acetylcysteine) show promise in some perioperative and critical care trials, but results are inconsistent. Mitochondria‑targeted antioxidants (like MitoQ, which came out of New Zealand research) are intriguing, not standard of care yet.
- Xanthine oxidase inhibitors (allopurinol) and NO donors/nitrite have signals in small studies and animal models; not routine for acute reperfusion outside trials.
| Scenario | Suggested SpO2 Target | PaO2 (if ABG available) | Notes |
|---|---|---|---|
| Acute MI (normoxemic) | 92-96% | 60-80 mmHg | No routine oxygen if SpO2 ≥ 90%; DETO2X‑AMI neutral, AVOID suggested harm with hyperoxia |
| Post‑ROSC (cardiac arrest) | 92-96% | 60-100 mmHg | Wean from FiO2 1.0 quickly; avoid PaO2 > 150-200 mmHg |
| Ischemic stroke (no hypoxia) | 94-96% | 70-90 mmHg | Supplement oxygen only if SpO2 < 94%; routine oxygen neutral in SO2S |
| COPD exacerbation | 88-92% | 50-70 mmHg | Avoid CO2 retention; titrate carefully, confirm with ABG |
| Post‑op ICU/mechanical ventilation | 92-96% | 60-90 mmHg | Prefer PEEP over high FiO2; long hyperoxia linked to harm |
| Neonatal resuscitation (term) | Use age‑in‑minutes targets | Not routinely used | Start room air (21%); titrate to nomograms; avoid hyperoxia |
| Neonatal resuscitation (preterm) | Use age‑in‑minutes targets | Not routinely used | Start 21-30%; adjust frequently to oximetry |
Guideline signals you can trust (without memorizing links):
- AHA/ILCOR/ERC 2020-2022: after ROSC, avoid hyperoxia; target normal saturations.
- AHA/ESC 2019-2023 (ACS): no routine oxygen if SpO2 ≥ 90-92%.
- AHA/ASA 2019-2021 (stroke): treat hypoxia; don’t add oxygen if normoxic.
- ANZCOR (Australia-NZ): routine oxygen is not needed in normoxemic ACS or stroke; use 88-92% targets in COPD.
- Neonatal resuscitation councils (ILCOR/ANZCOR): start in air (term) or low FiO2 (preterm); titrate to time‑based targets.
Checklist, Pitfalls, and Mini‑FAQ (Plus Next Steps)
Quick checklist for reperfusion moments
- Write the saturation target before/at reperfusion (e.g., 92-96%).
- Use oxygen to fix hypoxemia, not to polish a number.
- Step down FiO2 early; recheck ABG 10-20 minutes after flow returns.
- Prefer PEEP to FiO2 if you need support.
- Bundle: normothermia, glucose control, blood pressure support, pain/anxiety control.
- Document the wean plan in handovers.
Common pitfalls
- Parking at FiO2 1.0 after ROSC “just in case.” Fix it as soon as SpO2 is reliable.
- Ignoring the ABG because the pulse ox reads 100%. That can mask PaO2 > 250 mmHg.
- Overcorrecting COPD to 99%. Aim 88-92% unless unstable.
- Chasing a perfect number while neglecting flow. Oxygen can’t replace cardiac output.
- Forgetting temperature. Fever multiplies oxidative injury.
Heuristics you can use today
- If SpO2 is ≥ 94% on room air, do not add oxygen for ACS or stroke.
- After ROSC, reduce FiO2 every 1-2 minutes until SpO2 is 92-96%.
- Any PaO2 above ~120 mmHg in a reperfusion window is a nudge to lower FiO2.
- Use PEEP of 5-8 cm H2O before increasing FiO2 beyond 0.6, unless contraindicated.
- When you release a tourniquet or vascular clamp, be ready with ABG and vasopressors-but keep FiO2 modest.
Mini‑FAQ
- Isn’t more oxygen always safer in emergencies?
Not once you have a stable airway and measurable SpO2. In the first minute, sure-during intubation or arrest care, FiO2 1.0 is fine. The error is forgetting to dial down once flow returns. - What about hyperbaric oxygen (HBO)?
HBO has roles (carbon monoxide poisoning, gas embolism, some crush injuries), but not routine MI, stroke, or general I/R. The ROS hit can be worse if used indiscriminately. - Do antioxidants solve this?
Not reliably. Some perioperative and ICU studies suggest benefit (e.g., high‑dose vitamin C), but others don’t. None replace good oxygen titration. - Is “hypoxic reperfusion” a thing?
In the lab, starting with lower oxygen and ramping up reduces ROS. Clinically, we translate that into “avoid hyperoxia” and staged clamp release, not intentional hypoxemia. - How fast should I wean?
Very fast after ROSC or successful reperfusion-seconds to a few minutes-as long as SpO2 holds in range and hemodynamics are stable. - What if the pulse ox is unreliable?
Dark skin, shock, nail polish, motion, or dyshemoglobins can fool it. Get an ABG and consider forehead or ear probes.
Next steps by role
- Paramedics: Start high if needed, but set a target and drop quickly once you have a strong waveform. Hand over the target aloud.
- ED/ICU clinicians: Write an oxygen order with a saturation range. Add an ABG time. Pair oxygen changes with temperature and glucose control.
- Anesthetists/Surgeons: Use controlled reperfusion (gradual release, pressure support), keep FiO2 moderate, and plan for the 10-30‑minute window post‑release.
- Quality leads: Add “FiO2 at 10 minutes post‑reperfusion” to your audit board; it changes behavior.
- Researchers: Push pragmatic trials on staged oxygen targets and mitochondria‑targeted therapies in MI, stroke, and limb I/R.
Troubleshooting scenarios
- SpO2 stuck at 90% on FiO2 0.4: Increase PEEP to 8, reassess. If still low, consider recruitment maneuvers, check for edema/aspiration, then bump FiO2 in small steps.
- SpO2 100% with PaO2 260 mmHg: Drop FiO2 by 10-20% every couple of minutes; aim for PaO2 < 100 mmHg if feasible, SpO2 94-96%.
- Hypotension on tourniquet release: Treat with fluids/pressors as needed, keep FiO2 modest, and get an ABG (watch K+, lactate, pH).
- Post‑ROSC shivering pushing up oxygen need: Control temperature and shivering (sedation, analgesia, consider neuromuscular blockade) instead of cranking FiO2.
The take‑home is simple but not easy: give enough oxygen to reverse hypoxemia, then stop. Most of the harm sits in the first stretch after flow returns and in the habit of leaving FiO2 high because it feels safe. It isn’t. Good targets, quick weans, and a couple of ABGs do more to protect the heart, brain, and kidneys than any fancy antioxidant you can order today.




Pradeep Meena
September 6, 2025 AT 13:01Everyone talking about oxygen like it's magic but no one mentions how hospitals in India just pump 100% O2 into every patient after ROSC because they don't know better. We're not saving lives here we're just following habit. I've seen patients with SpO2 at 98% on room air get cranked to 100% and then crash because of oxidative stress. This post is right but nobody listens.
Rishabh Jaiswal
September 6, 2025 AT 22:43yo i read this whole thing and honestly its sooo true but like u know what the real problem is? nurses and docs are lazy. they just leave the oxygen at 100% and walk away. i work in er and last week a guy came in with mi sp02 96% on room air and the paramedic gave him 15lpm o2 and the nurse just kept it on. no one even checked the abg. we need to stop treating oxygen like a comfort blanket
May Zone skelah
September 7, 2025 AT 10:30Oh my god. This is the most profound, elegantly articulated, and clinically devastating critique of our oxygen dogma I've ever encountered. The way you framed the mitochondrial electron leak as a 'spring being wound tight'-it's not just science, it's poetry. And the fact that we've been treating oxygen like a panacea while quietly poisoning reperfused tissue? It's a collective moral failure disguised as protocol. I'm weeping. Not just for the patients, but for the entire medical culture that mistakes intensity for intelligence. Bravo. This should be required reading in every med school, every ICU, every cath lab from Boston to Bali.
Dale Yu
September 7, 2025 AT 22:22you think this is new? we've known this since the 90s. the problem isn't the science its the system. hospitals make money off high flow oxygen and ventilators and monitoring. they dont want you weaning it fast. they want you keeping patients on 100% so they can bill for 'complex respiratory support'. this isn't medicine its corporate healthcare with a stethoscope. stop pretending we're saving lives when we're just feeding the machine
Kshitij Nim
September 8, 2025 AT 06:43Great breakdown. I've been pushing this exact protocol in our cath lab for a year now. We started with a simple checklist: 'Target 92-96%, step down FiO2 every 2 min, ABG at 10 min.' The first month was rough-nurses were scared. But now we've cut hyperoxia events by 70% and no one's had a worse outcome. The key? Show them the data, don't just tell them. And always lead by example. If you walk in with FiO2 at 0.4 and SpO2 at 95%, they'll follow. It's not about being right-it's about making it easy for others to do the right thing.
Scott Horvath
September 9, 2025 AT 02:53man i just read this after a 12 hour shift and i swear i felt seen. been doing this for 15 years and i always felt weird about cranking o2 to 100% just because i could. now i know why. i dont need to be a hero with the oxygen knob. i just need to be smart. weaning fast feels scary at first but its like turning down the heat after the soup boils. you dont keep it on max forever. thanks for the clarity. gonna print this and stick it on my monitor
Armando Rodriguez
September 9, 2025 AT 20:26This is an exemplary piece of clinical guidance-clear, evidence-based, and actionable. The integration of trial data with practical bedside protocols demonstrates not only deep expertise but also a commitment to patient-centered care. I have already shared this with our ICU team and will be incorporating the checklist into our standard reperfusion protocol. The emphasis on documentation, ABG confirmation, and staged weaning aligns perfectly with our quality improvement initiatives. Thank you for elevating the standard of care with such precision and integrity.
jennifer sizemore
September 10, 2025 AT 19:10Thank you for writing this. I’ve seen so many patients get hurt by well-meaning but misguided oxygen use. I’m a nurse in the ER and I’ve had to fight to lower FiO2 on patients who were perfectly fine on room air. It’s exhausting. But reading this makes me feel less alone. I’m going to start handing this out to new residents and med students. We don’t need to fix what isn’t broken. Sometimes, the most powerful thing we can do is… nothing. Just watch. Just wait. Just breathe with them.