
When your kidneys start acting up-swelling, fatigue, less urine, weird lab results-it’s easy to blame a UTI or dehydration. But if you’ve been on common medications like omeprazole, ibuprofen, or amoxicillin for months or even years, there’s a hidden risk you might not know about: acute interstitial nephritis. It’s not rare. It’s not exotic. And it’s rising fast.
What Exactly Is Acute Interstitial Nephritis?
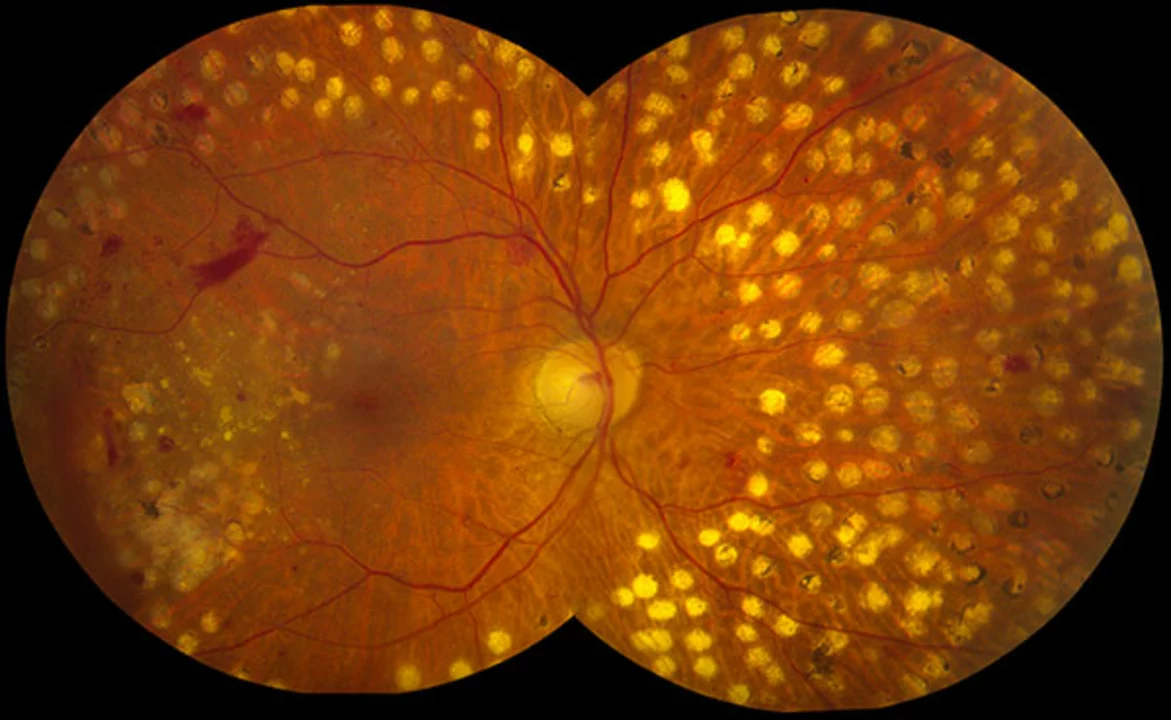
Acute interstitial nephritis (AIN) is when the space between your kidney’s filtering tubes becomes inflamed. That space, called the interstitium, supports the tiny tubules that clean your blood. When immune cells flood in-usually because of a drug-you get swelling, scarring, and a sudden drop in kidney function. It’s not the same as a kidney infection or glomerulonephritis. This is a quiet, sneaky reaction that doesn’t always show classic symptoms.
Think of it like an allergic reaction, but inside your kidneys. Your body mistakes a medication for a threat and sends in white blood cells, eosinophils, and other immune players to fight it. The result? Kidney damage that can look like acute kidney injury on blood tests. In fact, AIN causes 5 to 15% of all cases of sudden kidney failure in hospitals.
Which Drugs Are Most Likely to Cause It?
Over 250 medications have been linked to AIN. But three classes stand out-and they’re all things millions of people take daily.
- Proton pump inhibitors (PPIs) like omeprazole, esomeprazole, and pantoprazole: These are the new #1 trigger. Used for heartburn, they’re taken for years without a second thought. But in recent years, they’ve overtaken antibiotics as the most common cause. About 12 out of every 100,000 people on PPIs develop AIN each year. And here’s the kicker: even after stopping the drug, only 50-60% of patients fully recover kidney function.
- Antibiotics like penicillin, amoxicillin, ciprofloxacin, and sulfonamides: These used to be the top offenders. They cause AIN faster-often within 10 days-and come with classic signs like fever, rash, and high eosinophils. But recovery is better: 70-80% of patients bounce back fully if caught early.
- NSAIDs like ibuprofen, naproxen, and diclofenac: These are the sneaky ones. They account for nearly half of all drug-induced AIN cases. People on long-term NSAIDs-often for arthritis or chronic pain-are at highest risk. The problem? These drugs don’t usually cause rash or fever. Instead, they cause heavy proteinuria (over 3 grams a day), and recovery is slower and less complete. Nearly 42% of NSAID-induced AIN cases lead to permanent kidney damage.
Even newer drugs like immune checkpoint inhibitors (used in cancer therapy) are now being linked to AIN, though they’re still rare. The real danger? Polypharmacy. If you’re on five or more medications, your risk jumps 3.2 times. Age matters too. People over 65 are nearly five times more likely to develop AIN than younger adults.
Why Is It So Hard to Diagnose?
AIN doesn’t scream for attention. There’s no single blood test or urine dipstick that confirms it. The classic triad-rash, fever, and eosinophilia-shows up in less than 10% of cases. Most patients just feel tired, lose their appetite, or notice they’re peeing less. Doctors often mistake it for a urinary tract infection, dehydration, or even the flu.
Patients report waiting 2 to 4 weeks before getting the right diagnosis. One case from the American Kidney Fund tells the story: a 63-year-old woman took omeprazole for 18 months, then suddenly couldn’t urinate. She was hospitalized, put on dialysis for three weeks, and still had only 45% of her kidney function left a year later. She wasn’t told the drug could do this.
The only way to be sure? A kidney biopsy. That’s right-inserting a needle into your kidney to pull out a tiny tissue sample. It’s invasive, scary, and not always done quickly. But without it, you’re guessing. Tests like eosinophiluria or gallium scans aren’t reliable enough. And by the time you get to biopsy, you might already have lost months of kidney health.

Recovery: It’s Not Guaranteed
Stopping the drug is step one-and it’s non-negotiable. If you’re on a PPI or NSAID and your kidney function drops, your doctor should pull it immediately. Delaying by more than 48 hours reduces your chance of full recovery.
But stopping the drug doesn’t mean healing. Recovery timelines vary wildly:
- Antibiotic-induced AIN: Median recovery in 14 days. Most people bounce back fully.
- NSAID-induced AIN: Takes about 28 days. Only about half recover completely.
- PPI-induced AIN: Takes 35 days on average. Only 50-60% recover fully.
And here’s the hard truth: 30% of all AIN patients develop chronic kidney disease within a year. That means lifelong monitoring, diet changes, and possibly future dialysis. NSAID users are the most likely to end up here-42% develop stage 3 or worse CKD.
Some patients get steroids. Prednisone or methylprednisolone, given for 2-4 weeks, then slowly tapered. But here’s the controversy: no large randomized trials prove steroids work. Still, experts like Dr. Ronald J. Falk say they help in severe cases-especially when eGFR drops below 30 or kidney function keeps worsening after stopping the drug.
What Does Recovery Really Feel Like?
Patients who recover describe it like waking up from a fog. Energy returns. Swelling goes down. Urine output normalizes. But for others, recovery is incomplete.
A Medscape survey of 120 AIN patients found:
- 65% felt better within 72 hours of stopping the drug.
- 42% still had reduced kidney function (eGFR under 60) six months later.
- One in five needed dialysis for 2-6 weeks.
Many never realize their kidneys are permanently damaged. They feel fine. Their labs are “stable.” But eGFR doesn’t bounce back to normal. That’s chronic kidney disease. And it’s silent until it’s advanced.

How to Protect Yourself
You don’t need to avoid all medications. But you need to be smarter.
- Know your meds. If you’re on a PPI for more than 3-6 months, ask your doctor if you still need it. Many people take them years longer than necessary.
- Track kidney health. If you’re on NSAIDs or PPIs long-term, get a basic kidney panel (creatinine, eGFR) every 6-12 months. Don’t wait for symptoms.
- Don’t ignore vague symptoms. Fatigue, nausea, reduced urine, unexplained swelling? Don’t assume it’s aging or stress. Get your kidneys checked.
- Speak up about polypharmacy. If you take five or more medications, ask your doctor to review them. Are any unnecessary? Could any be replaced?
- Ask about biopsy. If your kidney function drops suddenly and no clear cause is found, insist on a biopsy. Early diagnosis saves kidneys.
What’s Next for AIN?
Research is moving fast. Scientists are testing urine biomarkers like CD163, which in one 2022 study showed 89% accuracy in detecting AIN without a biopsy. If validated, this could change everything-no more invasive procedures for suspected cases.
Meanwhile, the FDA and global health agencies are warning about PPIs. Between 2011 and 2020, over 1,200 cases of AIN were reported to the FDA. The number of cases has risen 27% since 2010, mostly because of increased PPI use.
If current prescribing trends continue, AIN cases could rise 15% by 2025. That’s not a prediction. That’s a projection based on data we already have.
This isn’t just about one rare kidney disease. It’s about how we use common drugs. It’s about trusting symptoms. It’s about asking the right questions before the damage is done.
Can acute interstitial nephritis be reversed?
Yes, but only if caught early and the triggering drug is stopped quickly. About 70-80% of patients recover kidney function fully if treatment starts within 7 days of symptoms. But if diagnosis is delayed beyond 14 days, the chance of full recovery drops by 35%. Some patients, especially those with NSAID-induced AIN or long-term PPI use, may have permanent kidney damage even after stopping the drug.
Are proton pump inhibitors (PPIs) safe for long-term use?
Long-term PPI use carries risks, including acute interstitial nephritis, bone loss, vitamin B12 deficiency, and gut infections. While many people benefit from short-term use (4-8 weeks), taking them for months or years without medical supervision increases AIN risk significantly. The FDA has issued safety warnings, and experts recommend reassessing PPI use every 3-6 months. If heartburn is controlled, consider tapering off.
Does AIN always require a kidney biopsy?
Yes, for a definitive diagnosis. Blood tests and urine analysis can suggest AIN, but they can’t confirm it. Other conditions like glomerulonephritis or obstruction look similar. A biopsy is the only way to see the immune cell infiltration in the kidney tissue. While new urine biomarkers like CD163 show promise, they’re still in research and not yet standard practice.
How long does it take to recover from AIN?
Recovery time depends on the drug that caused it. Antibiotic-induced AIN usually improves within 14 days after stopping the drug. NSAID-induced cases take about 28 days. PPI-induced AIN is the slowest, with median recovery at 35 days. Some patients need dialysis for 2-6 weeks. Full recovery can take months, and not everyone regains all kidney function.
Can I take NSAIDs again after having AIN?
No. Once you’ve had NSAID-induced AIN, you should avoid all NSAIDs permanently. Re-exposure can trigger the same reaction, often more severely. Even low doses or short courses carry risk. Acetaminophen (Tylenol) is the safer alternative for pain relief. Always inform all your doctors about your history of AIN.
Is AIN common in younger people?
It’s rare in people under 45. The incidence jumps sharply after age 65, with 22 cases per 100,000 in older adults compared to just 5 per 100,000 in younger adults. This is largely due to higher medication use, more chronic conditions, and age-related kidney changes. But younger people on long-term PPIs or multiple drugs are still at risk-just less likely.



Andrew Forthmuller
November 11, 2025 AT 02:03Just stopped my omeprazole after reading this. My creatinine was up last month. No symptoms, just a lab result. Scared the hell out of me.
dace yates
November 12, 2025 AT 21:41I’ve been on ibuprofen for my back for 5 years. No one ever told me this could happen. I’m scheduling a kidney panel this week. Thanks for laying it out so clearly.
Danae Miley
November 13, 2025 AT 15:30Let’s be precise: PPI-induced AIN is not "rising fast"-it’s exploding. The FDA’s own data shows a 27% increase since 2010, and PPI prescriptions have increased 120% in the same period. This isn’t correlation; it’s causation masked by overprescribing. And no, "just stop the drug" isn’t enough-most patients don’t even know they’re at risk until their eGFR is in the toilet.
Charles Lewis
November 14, 2025 AT 03:33It is important to recognize, from a clinical and public health perspective, that the phenomenon of drug-induced acute interstitial nephritis represents not merely an individual medical concern, but a systemic failure in medication stewardship. The widespread, often indefinite, use of proton pump inhibitors and NSAIDs-drugs that were originally intended for short-term, symptom-based intervention-has normalized chronic pharmacological exposure in populations without adequate monitoring protocols. The absence of routine renal function screening for patients on long-term regimens is, frankly, indefensible. We have the tools: creatinine, eGFR, urinalysis. We have the data: 5-15% of hospital-acquired AKI cases stem from AIN. What we lack is the will to implement preventive care at scale. Until primary care providers are incentivized to de-prescribe rather than prescribe, this epidemic will continue to grow.
Renee Ruth
November 15, 2025 AT 10:26My aunt got dialysis after taking omeprazole for "heartburn" for 7 years. She didn’t even know her kidneys were failing. Now she’s on a transplant list. And the doctor? Said "it’s just aging." Like that’s an excuse. This is medical negligence wrapped in a pill bottle.
Samantha Wade
November 16, 2025 AT 18:21This is exactly why we need mandatory medication reconciliation in primary care. Every patient on long-term PPIs or NSAIDs should have a kidney function review every 6 months-period. And pharmacists should be required to flag high-risk combinations. We’re not asking for miracles. We’re asking for basic safety protocols. This isn’t theoretical. It’s happening to people we know. Let’s stop pretending it’s rare.
Elizabeth Buján
November 16, 2025 AT 22:05i just read this and felt like someone punched me in the gut… i’ve been on naproxen for 8 years for my arthritis and never thought twice. i thought my tiredness was just getting older. now i’m scared to look at my last blood work. but also… thank you. this is the kind of info people need to hear before it’s too late.
vanessa k
November 18, 2025 AT 21:07I’m so glad someone finally said this. My dad was told his kidney issues were "just old age" until he got a biopsy. Turns out it was his daily ibuprofen. He’s been off it for a year and his eGFR is still at 48. He’ll never get it back. We’re all just guessing with these meds. No one warns us.
manish kumar
November 19, 2025 AT 12:10As someone who works in public health in India, I see this every day. People buy NSAIDs over the counter without prescription. They take them for months. No one checks kidney function. No one asks about their meds. This isn’t just an American problem-it’s a global silent crisis. We need community education, not just hospital biopsies. People need to know that a pill for heartburn can kill their kidneys slowly.
Nicole M
November 20, 2025 AT 04:43Wait so if I stop my omeprazole, will my kidneys actually heal? Or is the damage permanent? I’ve been on it for 4 years.
Arpita Shukla
November 21, 2025 AT 10:45You’re all missing the point. The real issue is that doctors don’t educate patients. But patients also don’t read the damn pamphlets. If you’re taking a drug for more than 6 months, you should be researching it yourself. It’s not the drug’s fault-it’s your ignorance. I’ve read the FDA warnings. You should too.
Benjamin Stöffler
November 23, 2025 AT 09:49But… what if… the interstitium… is not just a space… but a sentient membrane… that feels the chemical invasion… and retaliates… with the fury of a thousand immune cells…? Is AIN… not a rebellion… not a side effect… but a cry for help… from the body… that we’ve drowned in pills…?
Amber O'Sullivan
November 24, 2025 AT 20:08My nephrologist said if I’d waited another two weeks to get the biopsy I’d be on dialysis for good. Stop the drug. Get the biopsy. No excuses. Period.
Lashonda Rene
November 24, 2025 AT 23:20i never knew this could happen from just taking pills for heartburn. i thought it was just something that happened to old people in hospitals. now i’m scared to even take tylenol. but i’m gonna ask my doctor about my meds. this changed my whole perspective.
Samantha Wade
November 25, 2025 AT 15:10Thank you for sharing your story, @3867. That’s exactly why we need to push for mandatory kidney screening for anyone on long-term NSAIDs or PPIs. This isn’t fearmongering-it’s prevention. And if your dad’s eGFR is still at 48, he’s in stage 3 CKD. He needs a nephrologist, not just a GP. Let me know if you need help finding one.